Twin Co-Bedding
What is co-bedding and what guidance is available?

Twin sleep – including twin sleep safety, twin co-bedding, twin sleep patterns, and the impact of twins on parents’ sleep – is relatively under-researched. On this page we summarise the research which has been done.
Whilst Sudden Infant Death Syndrome (SIDS) is extremely rare, the rate is two-to-four times higher in twins, compared to singleton babies (Damato et al., 2016). This is likely to be because many more twins are born premature and/or at a low birth weight – factors which are both associated with increased SIDS risk in all babies.
It is important that parents are aware of how the sleep environment of twins can influence the risk of SIDS, as well as it’s effect on babies’ sleep, and ease of night-time care.
What is co-bedding and what guidance is available?
What positions do twins assume when sleeping on the same surface?
Considerations when co-bedding your multiples.
Twins are often born early and tend to follow a sleep trajectory that aligns more closely with their gestational age.
What is the disruption to parental sleep like with twins as opposed to singletons?
What is the available bed-sharing guidance for twin sleep?
Co-bedding is when both twins sleep together in the same cot. Studies done on twin co-bedding safety found no evidence to support that twins disturbed each other, overheated, or suffocated due to each other’s presence (Ball, 2006; Hayward et al., 2015). Hayward et al (2015) found co-bedding preterm twins had fewer adverse health issues and longer durations of quiet sleep than non-co-bedding preterm twins. Co-regulation of infant heartbeats means that co-bedding infants have significantly lower heart rates and thus have a lower stress levels overall (Hayward et al., 2015; Byers et al., 2003).
It is worth thinking about how to arrange furniture in the bedroom to make sure your twins can sleep in the same room as you for at least for six months from birth. Co-bedding may be one useful option.
Studies from New Zealand, the US, and UK found that co-bedding becomes less frequently practiced as twins age (Hutchinson et al., 2010; Damato et al., 2012; Ball, 2007). Roughly 50% of twin pairs co-bed at age 6 weeks, dropping to 30% at 4 months and 10% at 8 months of age (Hutchinson et al., 2010). As babies grow, co-bedding may become less common given the space constraints of sharing a cot.
In the US, the National Association of Neonatal Nurses’ position on co-bedding of twins and higher order multiples neither recommends nor warns against the practice, with the organisation emphasising the lack of sufficient body of knowledge (2012).
The American Academy of Pediatrics (AAP) recommends avoiding co-bedding twins for the same reason of insufficient data (Moon et al., 2022). However, AAP does not concentrate on healthy, full-term babies, and seems to overlook the outcomes of the research conducted by Ball.
NHS Choices (UK), on the other hand, advises that “You can put your twins to sleep in a single cot while they’re small enough. This is called co-bedding and is perfectly safe. In fact, putting twins in the same cot can help them regulate their body temperatures and sleep cycles, and can soothe them and their twin” (2025).
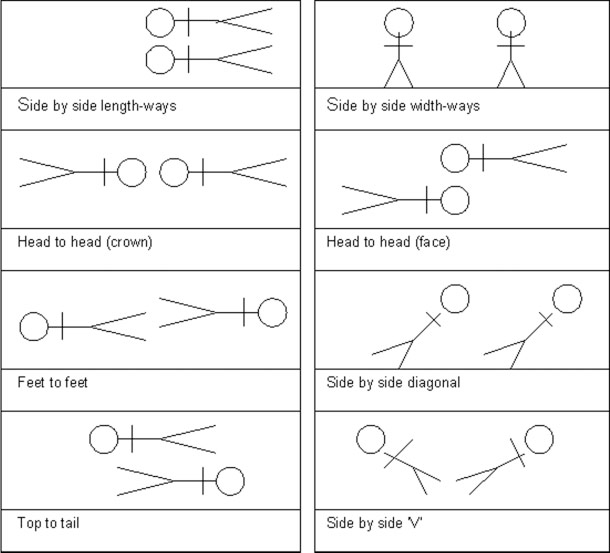
Studies carried out by Ball (2006) demonstrated that in the first month most co-bedded infants slept side-by-side. By the third month there was more variability, and those still co-bedded were positioned side-by-side, head-to-head and feet-to-feet. See the chart below of the various configurations reported by parents (Ball, 2006).
Of these various configurations, infants were found to continue to sleep safely in relation to each other unless obstacles were introduced (Ball, 2006). If babies are side by side widthways or positioned diagonally in the cot it is very difficult to secure covers, which introduces a potential hazard for infant safe sleep (Ball, 2006). If a baby sleeping bag is used for each infant, this issue is minimised. Read on to learn more about safe co-bedding with multiples.
While there is no strong evidence supporting co-bedding over separate bedding, or vice versa, general safe sleep advice applies to twins as well as singletons:
Twins Trust provides a diagram to help parents navigate safe sleep positions for multiples, which you can access here. Read on to learn more about the various ways twins position themselves when co-sleeping.
Research into the sleep patterns and duration of healthy twins is limited, as is evidence on how parents manage the sleep disruption that often accompanies caring for twins (Damato and Zupancic, 2009). However, the sleep patterns of twin babies are generally similar to those of singletons (Bartlett and Witoonchart, 2003). The key difference to consider is gestational age.
Twins are often born early and tend to follow a sleep trajectory that aligns more closely with their gestational age rather than their birth age. For this reason, comparing them to full-term singletons can be misleading. Prematurity, time spent in an incubator, and the transition home after a stay in a special care unit can all affect how twins sleep during the early weeks.
Environmental temperature can also impact sleep. Some families find that placing twins together helps them achieve more stable body temperatures and settle more easily. Premature twins may also need more frequent feeding due to smaller stomach capacity, which can result in more night wakings compared to full-term babies of the same chronological age.
Sleep development is individual and timelines vary, including for premature babies and/or twins. Read more about this variation on the infant sleep biology page.
There are two notable differences in how multiples are often cared for, compared to singletons:
While these strategies can help parents cope, they may also be challenging for babies who benefit from responsive and consistent care. Although research is limited, one approach supported by attachment theory is to keep primary caregiving with the parents where possible, and have helpers focus on practical support—such as household tasks, laundry, or making meals—rather than taking over baby care.
Chang (1990) interviewed parents of twins and found that inadequate sleep was the most commonly mentioned problem associated with caring for twin babies.
When it comes to night-time caregiving fathers are minimally affected by one infant, but have greater involvement when there are two. Studies have found that the night-time experiences of mothers – in terms of sleep disruption – were similar, regardless of whether they were caring for one infant or more (Ball, 2019).
For both fathers and mothers, the effects of prolonged sleep restriction include increased sleepiness, depression and decreased mental performance, together with a higher risk of illness and decreased ability to cope with demands. These contribute to an increased risk of postnatal depression with the mothers of twins known to be at increased risk post-partum, especially when coupled with difficulty falling asleep (Egsgaard et al., 2024). Fathers of twins were evidenced to have a slightly elevated risk of depression compared to fathers of singletons at the six month postpartum benchmark (Egsgaard et al., 2024). One way to help avoid postnatal depression is for parents to make a special effort to maintain their own normal circadian rhythms (read more about how to help cope with parental sleep disruption here).
The logically safest way to bed-share with twins is to have one baby in bed at a time, rotating them from a bedside cot (see image below). This allows one parent—often dad—to manage the rotation while mum rests and feeds. If both babies are in bed, placing them side-by-side with mum curled around the closer baby can work, rotating their positions for feeding. To prevent falls, ensure the outer baby is protected by a bedside crib or extra bed, not an open edge.

Avoid placing one baby on each side of mum, as she can’t monitor both at once. Some mothers tandem feed during the day, but doing so in bed requires sitting upright with pillows—which is not safe for sleeping. If lying down to feed both is the only way to manage night care, another adult should be present to monitor the babies and move them if mum falls asleep.
Last Reviewed: August 2025